27 de September de 2024
Acute Training Load – How to Measure & Interpret it
Why is it Important for Coaches to Monitor Acute Training Load
Updated coaches aim to pinpoint risk factors leading athletes to get injured while keeping an eye on and managing training variables to optimize sports performance. Training load stands as the crucial factor in boosting athletic performance, yet its imprecision can skyrocket injury risk. This training load encompasses the mechanical, physiological, and psychological load arising from multiple instances of physical activity by an athlete (Soligard et al., 2016).
A lack of control over training load will hinder athletes’ improvement, whether due to undertraining or overtraining. Another critical aspect to consider regarding this training variable is the abrupt change concerning the training load undertaken in the past, known as a spike in relative training load (Gabbett, 2016). To illustrate vividly, if our athlete is used to running about 60 kilometers and suddenly ramps up to completing 120 kilometers in a week, we’re doubling the training load. Such a blunder drastically heightens injury risk because of a sudden spike in relative training load.
To manage these shifts in training load, the term “acute:chronic workload ratio” (ACWR) was introduced in the literature in 2014 (Blanch & Gabbett, 2016; Hulin et al., 2014). The Acute Chronic Work Load Ratio or ACWR index was born to estimate the impact of weekly load on our athlete’s injury risk. This index assesses the correlation between recent (acute) training load vis-à-vis long-term past (chronic) training load and the risk of injuries. This article will delve into acute training load, but you can explore other topics on our blog focusing on chronic training load and their interrelation.
The Acute Chronic Work Load Ratio or ACWR index was born to estimate the impact of weekly load on our athlete’s injury risk. This index assesses the correlation between recent (acute) training load vis-à-vis long-term past (chronic) training load and the risk of injuries.

What is an Acute Training Load?
Monitoring acute training load ensures maximum athlete performance while drastically reducing the risk of injuries. Acute training load refers to the stress an athlete undergoes over a week, although some authors define it as the load of a single day (Bache-Mathiesen et al., 2023). Our player may have come from previous days of minimal training (chronic training load), not developing enough fitness for the tissue to tolerate the next levels of acute training load.
On the other hand, the athlete may have trained excessively in the preceding days, potentially damaging the tissue and not allowing enough time for it to regenerate before the next session or game. Each day, the athlete undergoes an acute training load, which can be measured as the load of that day or week, depending on the selected author. The coach’s objective in controlling acute training load is to have data on the fatigue and physical and mental tiredness accumulated by the player in relation to what they were doing.
Imagine a top-level professional basketball player who trains daily and covers a significant number of miles each week. This athlete is accustomed to that usual volume (chronic training load) and can slightly increase it the following week without much trouble. However, the soft tissues of an amateur basketball player are not adapted to such high volumes because they have a low chronic training load (not accustomed to high volumes). If we drastically increase the acute training load from one week to another, we significantly increase the risk of injury for that athlete.


Velocity Based Training 【 #1 VBT Guide in the World 】
How do We Measure Acute Training Load
The consensus in scientific literature indicates that acute training load accumulates over the past seven days, whereas chronic training load represents the average of the previous three to six weeks (Gabbett et al., 2016; Gabbett & Whiteley, 2017). Therefore, acute training load is established by collecting various parameters from a week of training and competition, such as internal loads (e.g., heart rate, session rating of perceived exertion [sRPE] × duration, measures of creatine or lactate…) and external loads (e.g., total distance, running speed and/or acceleration via global positioning systems [GPS], weight lifted, throws made…) (Malone et al., 2017).
It can also be obtained from self-reported questionnaires of fatigue, stress level, delayed onset muscle soreness (DOMS), and sleep quality/disorders. Analyzing both perceived load and well-being status can be interesting due to their potential to integrate different types of stimuli, as well as their ease of use and low cost (Clemente et al., 2019).
This section encompasses all the variables that the coach wants to measure as key indicators of performance in their sport. A baseball pitcher will need to analyze the number of pitches thrown, a sprinter should monitor the sprints performed at maximum intensity, and a powerlifter will need to analyze the sets performed for each movement and the intensity with which they were done. The ultimate goal of measuring acute training load is to measure everything that is measurable and useful for performance improvement and injury prevention.
Today, there are specific data analyst positions responsible for compiling all these GPS and technology data. These data shape the acute training load of each week, providing a simple and reliable tool for programming subsequent training weeks based on the average load of previous weeks (chronic training load). Each variable is measured differently and with specific technology. The idea of acute training load is to be able to measure the weight lifted that week, the kilometers covered, the perceived effort of the sessions, etc. These parameters are then used in the acute:chronic workload ratio to ensure that what we have done in the last week is not too far from what we were doing in the previous ones.

How is Acute Training Load Interpreted?
The acute training load is not a measure that is interpreted on its own. If you see data about a soccer player who has covered a certain distance at different speeds, or who has completed 9 sets of squats, it won’t tell you much. This measure becomes useful when compared with the chronic training load, which is the average of what has been done in previous weeks. The goal is for the acute training load to be lower, equal to, or slightly lower than the chronic load. Research suggests an acute:chronic workload ratio (ACWR) ranging between 0.8 and 1.3 (Malone et al., 2017; Windt & Gabbett, 2017). These numbers refer to the division of the acute training load by the chronic training load. It’s impossible and endless to delve into how each of the aforementioned variables is measured and calculated, so we should understand that the utility of measuring acute training load is to compare it with chronic training load.

To provide a simple example, if a long-distance runner has covered 80 kilometers this week (acute training load) and has been averaging around 100 kilometers in previous weeks (chronic training load), the ACWR ratio would be 0.8, obtained by dividing 80 km by 100 km. If this week we completed 100 kilometers and we have been averaging that in previous weeks, the ACWR ratio is 1, obtained by dividing 100 km by 100 km. The following figure from (Gabbett, 2016) shows the “sweet spot” highlighted in green in the ACWR ratio between 0.8 – 1.3. As that ratio increases, we move closer to the “danger zone” where the risk of injury exponentially increases.
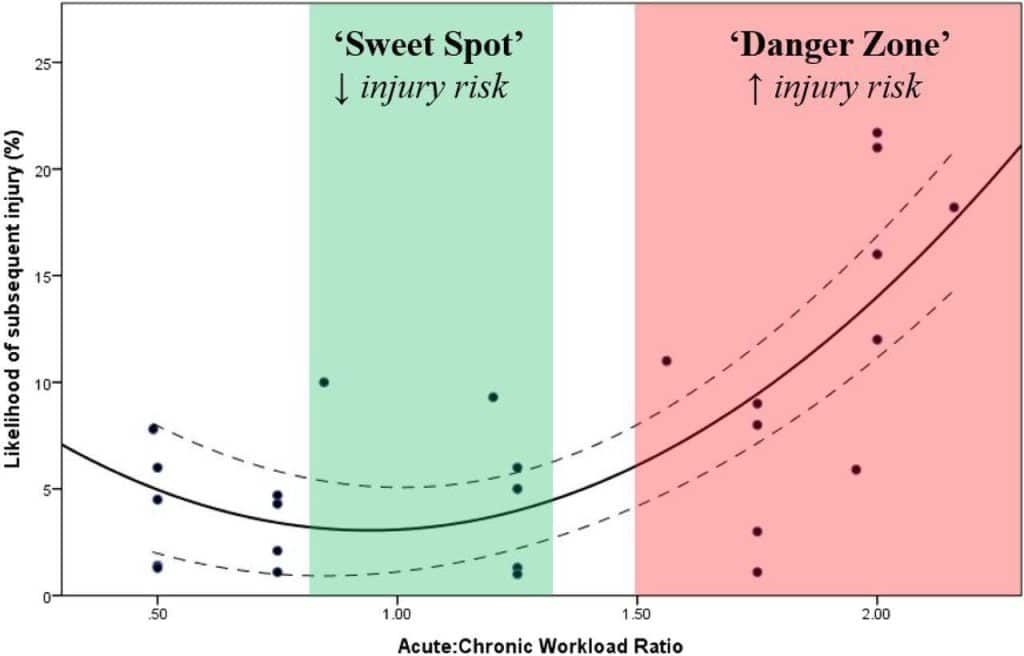
If the ACWR ratio is ≥ 1.5, it’s considered that the athlete is not well-prepared and likely has a higher risk of suffering acute injuries because the acute training load exceeds the chronic load by too much (Malone et al., 2017; Windt & Gabbett, 2017). Going back to the previous examples of a long-distance runner, if they run 150 kilometers this week (acute training load) and have been averaging 100 kilometers in previous weeks (chronic training load), the ACWR ratio will be 1.5. If the ACWR ratio is ≥ 1.8, the risk of injury drastically increases, even up to 50% higher (Gabbett, 2016).
The association between acute training load and chronic load provides valuable information for coaches to effectively manage the training process, achieve improvements, and prevent inadequate adaptations that can interfere with sleep quality, stress, and DOMS, thereby impairing performance and increasing the risk of injuries (Gabbett, 2016).
References
Bache-Mathiesen, L. K., Andersen, T. E., Dalen-Lorentsen, T., Tabben, M., Chamari, K., Clarsen, B., & Fagerland, M. W. (2023). A new statistical approach to training load and injury risk: separating the acute from the chronic load. Biology of Sport, 41(1), 119–134. https://doi.org/10.5114/BIOLSPORT.2024.127388
Blanch, P., & Gabbett, T. J. (2016). Has the athlete trained enough to return to play safely? The acute:chronic workload ratio permits clinicians to quantify a player’s risk of subsequent injury. British Journal of Sports Medicine, 50(8), 471–475. https://doi.org/10.1136/BJSPORTS-2015-095445
Clemente, F. M., Mendes, B., Bredt, S. D. G. T., Praça, G. M., Silvério, A., Carriço, S., & Duarte, E. (2019). Perceived Training Load, Muscle Soreness, Stress, Fatigue, and Sleep Quality in Professional Basketball: A Full Season Study. Journal of Human Kinetics, 67(1), 199–207. https://doi.org/10.2478/hukin-2019-0002
Gabbett, T. J. (2016). The training—injury prevention paradox: should athletes be training smarter and harder? British Journal of Sports Medicine, 50(5), 273–280. https://doi.org/10.1136/BJSPORTS-2015-095788
Gabbett, T. J., Hulin, B. T., Blanch, P., & Whiteley, R. (2016). High training workloads alone do not cause sports injuries: how you get there is the real issue. British Journal of Sports Medicine, 50(8), 444–445. https://doi.org/10.1136/BJSPORTS-2015-095567
Gabbett, T. J., & Whiteley, R. (2017). Two Training-Load Paradoxes: Can We Work Harder and Smarter, Can Physical Preparation and Medical Be Teammates? International Journal of Sports Physiology and Performance, 12(Suppl 2), 50–54. https://doi.org/10.1123/IJSPP.2016-0321
Hulin, B. T., Gabbett, T. J., Blanch, P., Chapman, P., Bailey, D., & Orchard, J. W. (2014). Spikes in acute workload are associated with increased injury risk in elite cricket fast bowlers. British Journal of Sports Medicine, 48(8), 708–712. https://doi.org/10.1136/BJSPORTS-2013-092524
Malone, S., Owen, A., Newton, M., Mendes, B., Collins, K. D., & Gabbett, T. J. (2017). The acute:chonic workload ratio in relation to injury risk in professional soccer. Journal of Science and Medicine in Sport, 20(6), 561–565. https://doi.org/10.1016/J.JSAMS.2016.10.014
Soligard, T., Schwellnus, M., Alonso, J. M., Bahr, R., Clarsen, B., Dijkstra, H. P., Gabbett, T., Gleeson, M., Hägglund, M., Hutchinson, M. R., Janse Van Rensburg, C., Khan, K. M., Meeusen, R., Orchard, J. W., Pluim, B. M., Raftery, M., Budgett, R., & Engebretsen, L. (2016). How much is too much? (Part 1) International Olympic Committee consensus statement on load in sport and risk of injury. British Journal of Sports Medicine, 50(17), 1030–1041. https://doi.org/10.1136/bjsports-2016-096581
Windt, J., & Gabbett, T. J. (2017). How do training and competition workloads relate to injury? The workload-injury aetiology model. British Journal of Sports Medicine, 51(5), 428–435. https://doi.org/10.1136/BJSPORTS-2016-096040